
It's undeniable that 99% of people spewing theories about nasolabial folds have no idea what they’re talking about. Cosmetologists and plastic surgeons regurgitate nonsense about bone recession, volume loss, or genetics when the reality is much simpler and if you don’t understand it you won’t be able to fix it.
So lets breakdown why nasolabial folds form and the actual methods to remove them.
THEORY VS. REALITY
The mainstream cope is that nasolabial folds come from:
1. Bone recession – Specifically, nasal aperture widening + deepening of the canine fossa.
2. Volume loss – Midface fat loss causing skin to “fall”
3. Bad bone structure – Weak forward growth leading to premature folds.
Which is FALSE.
If it were true, then:
• Why do people get nasolabial folds in their early 20s before any significant bone loss?
• Why do people with perfect forward growth still get them?
• Why are they universal across all ethnicities and phenotypes?
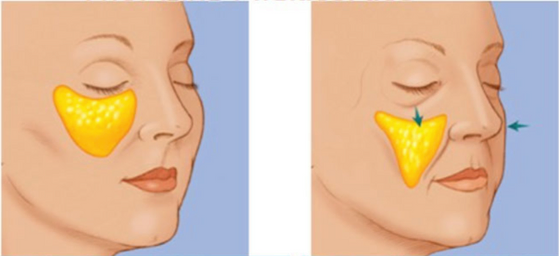
The answer is simple: gravity pulls midface fat downward, and the nasolabial fold is where it accumulates.
THE REAL CAUSE – GRAVITY & FAT MIGRATION
What’s actually happening:
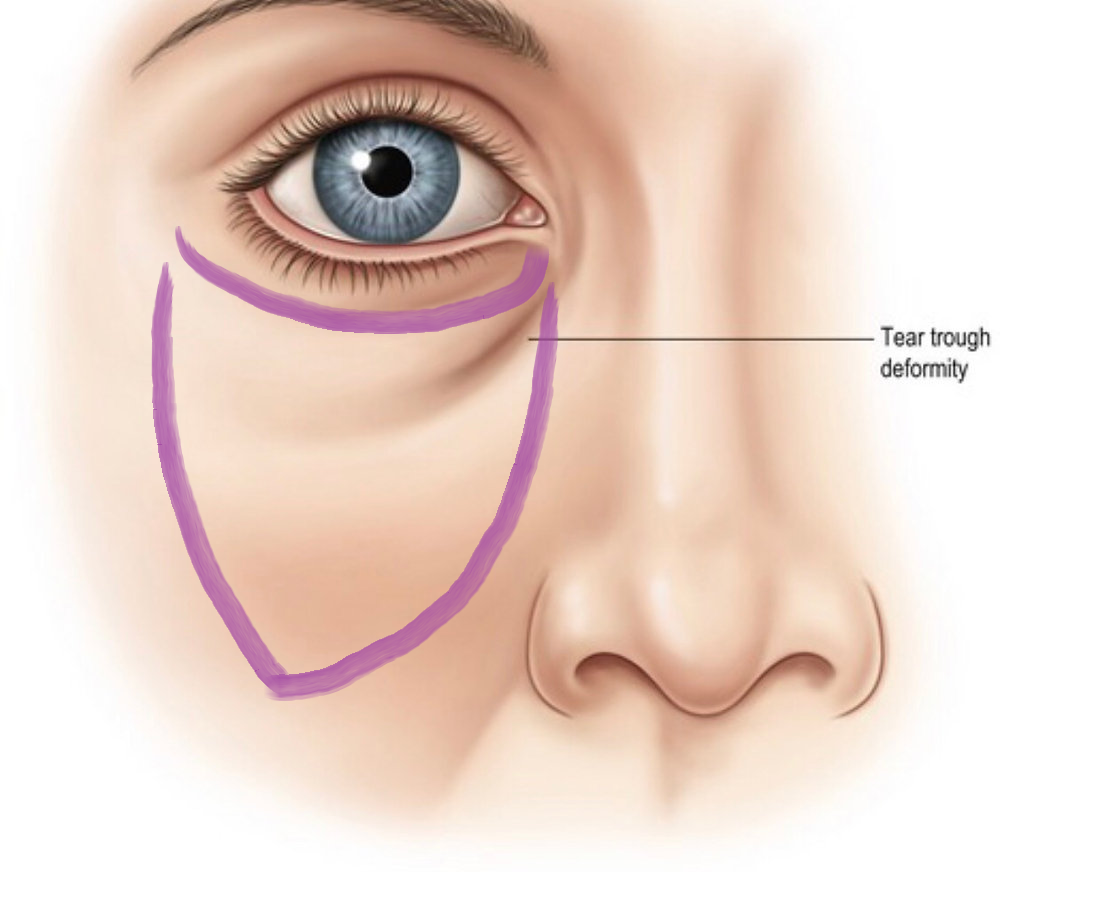
1. Fat starts migrating from the under eye and upper cheek.
2. It accumulates at the nasolabial fold because of anatomical resistance (thick superficial veins act as a barrier).
3. The result is the “crease” but not due to lost volume, but displaced volume.
Which perhaps explains why:
• Even people with perfect forward growth get them.
• Even people with full midface volume develop them.
• Surgical facelifts don’t fully fix them, because the issue isn’t skin laxity it’s the misplaced fat.
This also explains why PDO threads, collagen stimulation, or lifting techniques fail because they don’t address fat accumulation at the fold.
SURGICAL & NON-SURGICAL FIXES – WHAT ACTUALLY WORKS?
1. AQUALYX (DEOXYCHOLATE) FAT DISSOLVING – Best Non-Surgical Option
If fat has migrated to the fold, you dissolve it.
Procedure:
• Use Aqualyx (deoxycholate injections) directly into the nasolabial fold.
• Injection points: Spread 0.05ml per site, spaced ~1cm apart.

This is where you would inject it.
• Expect to look like a frog because of the swelling which will last for ~1 week post injection. Results visible in 2-3 weeks.
• Repeat every 3-4 weeks as needed.
Why this is legit:
• Removes fat at the accumulation site instead of trying to “lift” it back up.
• Targets the real problem instead of chasing volume loss copes.
(you can also do it for submental area~ a guide will be posted about it.)
2. MIDFACE FAT TRANSFER (If Volume Loss Exists)
Now in some cases the upper midface actually does lose volume as well so this needs to be corrected alongside fat dissolution.
Procwdures?
• Fat grafting to the midface/under eye region restores fullness where it belongs.
• HA fillers (temporary) or custom implants (permanent) can also be used.
• PDO threads, Sculptra, or other collagen inducing methods may help maintain skin tightness.
If you only dissolve fat without correcting lost volume you will simply risk a hollowed out look.
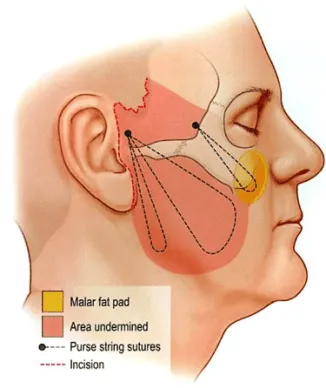
3. COMPOSITE FACE LIFT – The Only Surgical Fix That Works
Note: Standard facelifts do not fix nasolabial folds.
Why?
• They pull skin laterally, not vertically.
• The deep cheek fat remains in the nasolabial region.
What actually works:
• Composite facelifts (deep- plane techniques) lift the fat pad itself.
This is the only true surgical correction.
WHAT DOESN’T WORK (COPES)
🚫 Standard Midface Lift / S Lift – Doesn’t correct the fat migration only tightens skin.
🚫 PDO Threads – Temporary and does nothing for the fat pad itself.
🚫 Overfilling the Midface – Just makes you look retarded conns ridden goblin.
🚫 Skincare or Face Exercises – Completely utterly dogshit for structural issues.
FINAL VERDICT – HOW TO ACTUALLY FIX NASOLABIAL FOLDS
1 → Use Aqualyx (deoxycholate) to dissolve accumulated fat.
2 → Restore midface volume with fillers, fat grafting or implants (if needed).
3 → If necessary a composite facelift is the only surgical fix that fully resolves it.